

Our Origins
Pebble's capability was built over 25 years, beginning with observations. Patients were receiving care based on assumptions never rigorously tested, on evidence long since superseded, on techniques that persisted because they had always been done that way.
Surgical methods continued unchanged for decades while questions that could have been answered were not being asked, and technologies were adopted or rejected on the basis of studies too small to detect what mattered.
Behind this lay a deeper problem. The methods used to develop new therapies relied on models that could not predict human outcomes, on studies conducted in systems so far removed from human physiology that their findings failed to translate. Promising therapies failed in humans having succeeded in animals, while harmful therapies reached patients having appeared safe in models that could not detect the harm. From this emerged a conviction:
We will build something that could.

What We Built
We ran clinical trials and preclinical studies across countless programmes: drugs, devices, diagnostics, surgical techniques. Each one taught us what works and what fails.
We never worked in isolation. Collaborations developed across the UK, US, Sweden, Norway, Italy, and Australia. Professor Stig Steen (Igelösa, Sweden) was a major influence. His insistence on the tangible shaped everything that followed. But the capability we built is distinct: constructed through repetition until patterns emerged about what predicts human outcomes and why so much conventional preclinical research fails to translate.

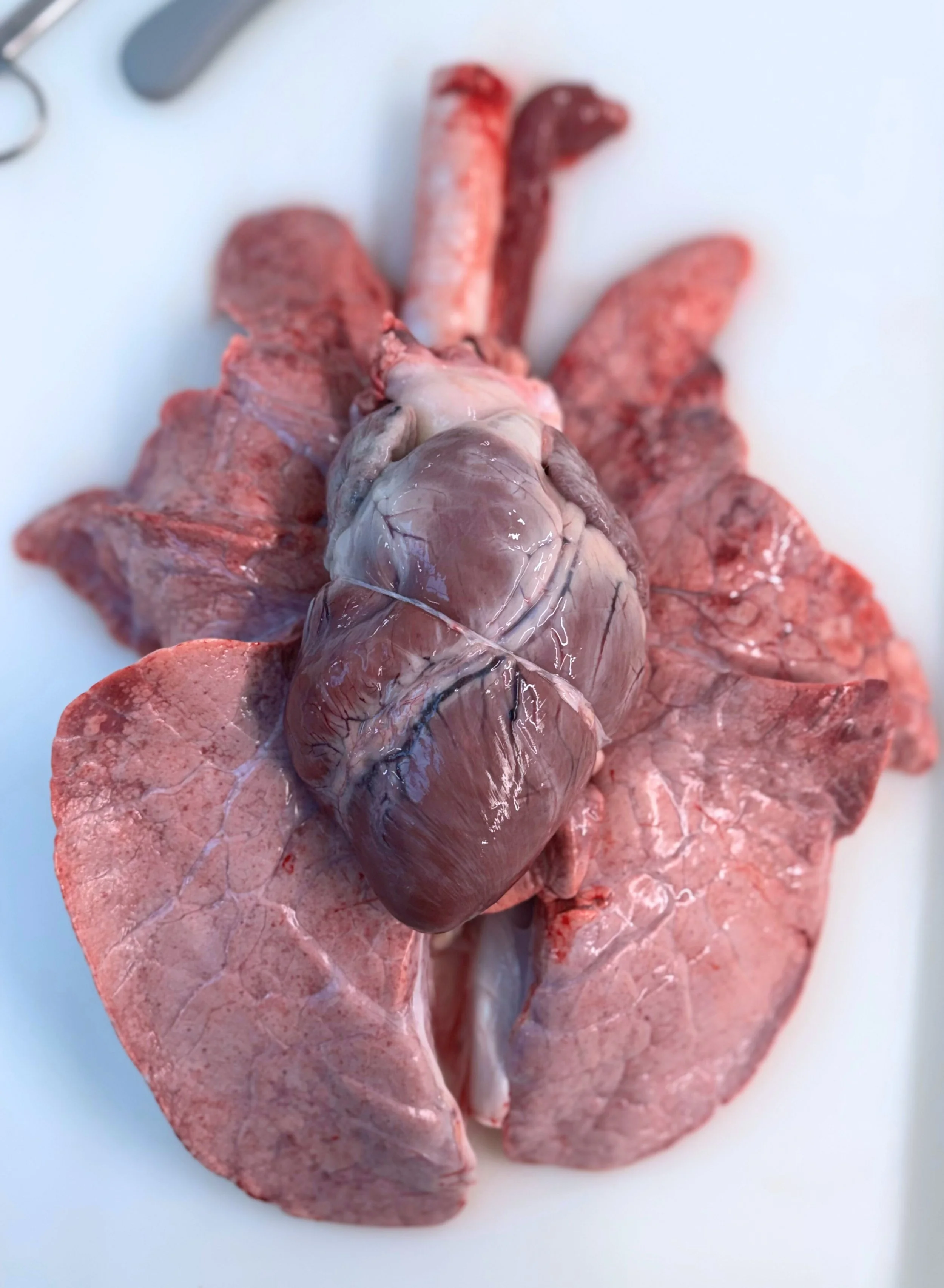
Today, Pebble operates from a 400-year-old dairy farm; state-of-the-art critical care infrastructure, hidden in plain sight. Over two decades we designed, built, validated, and refined the platforms that answer these problems: living organ systems that predict human responses, protocols tested through hundreds of procedures, and the hard-won expertise to know which questions matter and how to answer them.

We are not a contract research organisation. We do not execute protocols to specification. We solve difficult problems, generating solutions that would not emerge anywhere else.
This is governed by principles we do not compromise on and which shape everything we do. We do not accept every problem, only those where solving it will change practice and benefit patients. We do not accept every partnership, only those who can bring the solution to patients who need it. What we accept, we pursue until it changes practice.